Atrial Fibrillation
Non-persistent or paroxysmal atrial fibrillation is the most frequent sustained cardiac arrhythmia. Its increase is associated with the aging of the population.
It is an alteration of the normal conductivity of the heart (sinus rhythm), when the atria do not contract properly and the ventricles do so irregularly and excessively quickly, preventing the normal functioning of the heart.
A healthy heart, under normal conditions, should have a regular heart rhythm, since it is natural for it to accelerate only when we exercise, and slow down when we sleep. The normal heart rhythm ranges from 60 to 100 beats per minute and is called sinus rhythm. When arrhythmia appears, the normal rhythm of the heart is disturbed, it can accelerate despite being at rest (tachycardia) or slowing down (bradycardia).
AF appears when, under normal conditions, the heart rate is no longer regular and constant, the time between beat and beat is uneven. The fibrila heart (as if trembling).
Atrial fibrillation (AF) is the most frequent maintained arrhythmia in our day (with an estimated prevalence in the adult population between 0.4 and 2%), conditioned by a significant increase in mortality due to cardiovascular problems.
Atrial fibrillation Symptom
Patients usually present with palpitations, choking sensation, chest pain, fatigue, dizziness, dizziness. In general, atrial fibrillation is unable to perform the simple tasks of everyday life.
Throughout the course of the disease, the patient may experience symptomatic and asymptomatic periods, since, over time, palpitations may even disappear. This is important because you can be in danger without feeling any discomfort.
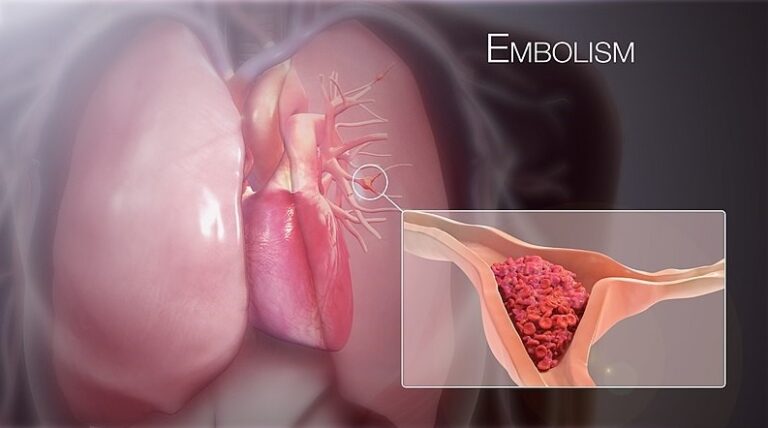
Loss of synchronicity in rhythm can cause formation of blood clots inside the heart, since when the heart goes into fibrillation the emptying of blood from the atria may not be total.
Occasionally, it is discovered that a patient has atrial fibrillation because he suddenly suffers from cerebral ischemia (transient or permanent), whose clinical manifestations (difficulty mobilizing half the body or speaking or both) could disappear within 24 hours or remain permanent (or even produce death).
Causes of atrial fibrillation
The appearance of atrial fibrillation can be associated with:
- Genetic predisposition.
- Arterial hypertension.
- Having suffered a myocardial infarction.
- Have undergone cardiac surgery.
- Diabetes.
- Heart valve disease.
- Congenital heart disease.
- Thyroid disease.
- Heart failure.
- Chronic lung disease.
- Sleep apnea.
- Alcohol abuse and stimulants.
- Emotional and physical stress
- Obesity.
- Lack of exercise (sedentary lifestyle).
It can occur both in hearts with previous pathology and in healthy hearts.
Depending on the duration of the episodes, it can be classified as:
Paroxysmal AF: It is short-lived (approximately 7 days), appears and disappears spontaneously.
Persistent AF: The arrhythmia does not go away by itself and lasts more than 7 days. It is necessary to take medications to control the heart rhythm, or resort to techniques such as cardioversion (controlled electric shock) so that the heart returns to its normal rhythm.
Chronic FA: It is long lasting. Arrhythmia does not stop with medication or controlled cardioversion.
Diagnosis
Electrocardiogram.
Only test needed to detect AF. It records the electrical activity of the heart and is a simple test and not painful. Its only drawback is that the AF has to be presented at the time the test is performed, so when the discomfort only appears on time, the diagnosis can be complicated.
Atrial fibrillation is characterized by the appearance of a chaotic and irregular rhythm in the atrium, of very high frequency, whose expression on the ECG is the appearance of F waves. QRSs are irregular due to the variable conduction block at the node level. . There are multiple impulses that reach the AV node, and most of them are not conducted (they are blocked). When the AV node is normal, and without treatment, the heart rate can range from 110-170 beats / min.
Holter
It is based on an electrocardiogram that records the functioning of the heart for 24 or 48 hours, while doing the usual activities. This allows detecting episodes of AF of short duration, or that do not cause symptoms.
-Echocardiogram.
Painless scan that allows to obtain images of the moving heart, to evaluate its shape, the state of the valves, atria and ventricles and their functioning. It also helps to detect many of heart disease that can cause AF.
Atrial fibrillation treatment
Treatment depends on the severity and frequency of symptoms and the existence or not of disease associated cardiovascular. The goal is to try to restore the normal heart rhythm (sinus rhythm):
- Cardioversion: Procedure to correct the arrhythmia and restore the normal rhythm of the heart. It can be done through antiarrhythmic drugs (pharmacological cardioversion) or, if they do not take effect, by electric shocks with a defibrillator (electric cardioversion).
- This last procedure requires general anesthesia and the taking of anticoagulant drugs before and after its application.
- Correct the situations that cause this arrhythmia (hypertension, Heart Failure) and control the risk factors.
- Ablation: A technique that consists of electrically isolating the pulmonary veins (where arrhythmia is born). To reach them, a catheter is inserted through the groin area (femoral vein) to the heart. Once there an electric current is generated that allows consecutive burns around of the pulmonary veins, being isolated or disconnected. It is performed with local anesthesia and sedation.
- Antiarrhythmic Drugs: They are classified into two types: those that try to return their normal rhythm to the heart and those that decrease the heart rate during the arrhythmia episodes. Its use is limited, due to its intermediate efficacy, aggravation of arrhythmia or toxicity and its tolerability. They can have side effects: heart rate too slow, fatigue, dizziness.
- Focused treatments to thrombus prevention, since AF increases the risk of stroke or stroke by 5 to 7 times.
- Anticoagulant drugs. They prevent the formation of clots and reduce the risk of thrombi forming within the blood vessels, delaying the time of blood clotting. There are two types of oral anticoagulants:
- Antivitamin K. They inhibit vitamin K, a substance involved in the coagulation process. Its effect can be altered by the diet and by the interaction with other medications, so periodic checks should be carried out every 4-6 weeks and the dose adjusted according to the INR result. The INR is the index that indicates the time it takes for blood to clot.
- Direct Oral Anticoagulants. They directly inhibit different coagulation factors. They are administered at fixed doses, without the need for periodic controls, since their effect is predictable and constant.
Complications of atrial fibrillation
The absence of atrial contractions predisposes to thrombus formation and the annual risk of cerebrovascular embolic events ranges around 7%.
Atrial fibrillation can also affect cardiac output; Loss of atrial contraction can reduce cardiac output at a normal heart rate by approximately 10%. Such a decrease is generally well tolerated, except when the ventricular rate becomes too fast (e.g.,> 140 beats / min), or when patients have cardiac output at a borderline or low value from the beginning. In these cases, it can evolve to heart failure.
When to consult the doctor
If you have any symptoms of atrial fibrillation, ask for a doctor’s consultation. The doctor may request an electrocardiogram to determine if the symptoms are related to atrial fibrillation or another heart rhythm disorder (arrhythmia). If you have chest pain, seek immediate medical attention immediately. Chest pain could be a sign that you are having a heart attack. Call now (586) 698-1200 to schedule an appointment with a Cardiologist in Sterling Heights, Washington Township or Rochester Hills, Michigan.